Heart Arrhythmia: Heart Rhythm Disturbances
Heart Arrhythmia: Heart Rhythm Disturbances
At heart arrhythmia, the normal heart rate is disturbed by various causes (Source). The heart then beats either too slowly (bradycardia) (Source), too quickly (tachycardia) or irregularly (arrhythmia) (Source). There are disturbances in the formation of electrical impulses that trigger a heartbeat (Source), and disturbances in the transmission of these impulses (Source). Read about the differences between these several heart rhythm disturbances and how to recognize them.
ICD codes for this disease: R00 I48 I46 I47 I49 I45 I44
Heart Arrhythmia: Where do they come from?
Normally, the so-called sinus node, a small area in the right atrium, generates electrical impulses for the heartbeat. They first spread across the atria, which then contract. Between the atria and the ventricles, there is a lot of connective tissue of the heart skeleton. It acts as electrical insulation. The impulses are thus only conducted into the ventricles at a special connecting node, the AV node.
From there, the charges travel along with the His bundle, the ventricular legs and the Purkinje fiber in the direction of and along the tip of the heart. From there, the heart muscle contracts and pumps the blood into the large bloodstream. heart arrhythmia can occur if the sinus node does not generate the electrical impulses properly, if the impulses are not transmitted properly, or if additional impulses are generated in the atrium or ventricle. There are dangerous and harmless heart arrhythmias.
How do I recognize a heart arrhythmia?
heart arrhythmias can cause various symptoms. Heart palpitations, heart stumbling, dizziness, chest pain, or fainting spells are among the typical signs. You can read more about this in the article Heart rhythm disturbances: Symptoms.
What are the Causes of Heart dysrhythmia?
You can read everything important about the causes of heart arrhythmia in the article heart arrhythmias: Causes.
Heart Arrhythmia: What Is It?
Heart arrhythmias can be divided into two main categories. If the heart beats too fast (more than 100 beats per minute), doctors speak of tachycardia. A heartbeat that is too slow (less than 60 beats per minute), on the other hand, is called bradycardia. However, doctors only see relevant bradycardia when the heart beats even slower (at least less than 50 beats per minute. It should not be forgotten that even many a well-trained heart athlete can beat so slowly without being ill.
An important term we utilize here is “arrhythmia“. By that, doctors mean irregular heartbeat with irregular heartbeat. If the heart beats too fast, it is called tachyarrhythmia. If the heartbeat slows down considerably, this is called bradyarrhythmia.
Ventricular arrhythmias
Heart arrhythmias are usually classified according to where they first occur. Changes in the heartbeat that originate in the ventricles are called ventricular arrhythmias. If the excitation is caused by this, it is called supraventricular arrhythmia.
Typical ventricular arrhythmias are
- Extra beats (ventricular extrasystoles)
- Ventricular flutter
- Ventricular fibrillation
- Ventricular tachycardia (e.g. torsade-de-point tachycardia)
Supraventricular arrhythmias
Supraventricular arrhythmias in particular are further classified in some places according to where pathological processes take place in the conduction system:
Normotopic or orthotopic stimulation disturbances are heart arrhythmias originating from the sinus node. The formation of the electrical impulses is altered, as is the case with:
- Sinus arrhythmia (e.g. the sick sinus syndrome)
- Sinus bradycardia (under 60 beats per minute, sometimes under 50 beats)
- Sinus tach
Heterotopic irritation disorders have their origin outside the sinus node. Then the impulses originate either in the atrial muscle itself, in the AV node, or in the “His” bundle. These include, for example:
- Extra strokes (extrasystoles)
- Atrial tachycardia (e.g. in the case of hyperthyroidism)
- Atrial fibrillation/flutter
- AV rhythm/extrasystole (as secondary pacemaker approx. 40-50 beats per minute)
- His-bundle rhythm/extrasystole (as tertiary pacemaker approx. 30-40 beats per minute)
Conduction disorders are present when the transmission of impulses from the sinus node via the AV node into the ventricle is disturbed, as in these clinical pictures:
- Sinuatrial Block (SA Block)
- Atrioventricular block (AV block)
- Intraventricular block (e.g. (in)complete right bundle branch block or/and left bundle branch block)
This also includes heart arrhythmias that occur in attacks (paroxysmal). In this case, some patients have additional “wires” for the electrical impulses.
- AV Node Reentry Tachycardia
- AV reentry tachycardia (additional conduction bundles as in WPW syndrome)
Resuscitation
If the heart stops beating at all, doctors speak of asystole. Sometimes there are still individual electrical discharges, which can also be seen in an ECG, called pulseless electrical activity (PEA). However, this is no longer sufficient for a heartbeat. As in ventricular tachycardia without pulse or ventricular fibrillation, PEA or asystole requires immediate resuscitation.
How dangerous are heart arrhythmias?
Some rhythm disturbances are harmless, others are life-threatening. If a heart arrhythmia lasts longer, it can have some consequences. For example, the heart becomes weaker and weaker (heart failure). The risk of heart attacks also increases. For example, a heart attack is imminent because fast-beating hearts consume more oxygen. The heart muscle gets this oxygen from the coronary arteries. If the coronary arteries or the heart muscle itself is abnormally altered, the oxygen supply will no longer be sufficient over time and there is a risk of an undersupply (ischemia).
With irregular and rapid heart arrhythmias, the blood swirls around in some places in the heart. If this condition persists, the blood clumps together and a thrombus develops. It can detach itself from the heart and migrates via the bloodstream to other parts of the body. There the vessels become increasingly narrow, so that the blood clot gets stuck and blocks the vein. As a result, the organ in question, or at least parts of it, is no longer supplied with sufficient oxygen and die. The consequences are a stroke in the brain, a pulmonary embolism in the lungs, or a renal infarction in the kidney with subsequent renal failure.
Heart arrhythmia In Sports
Especially in children and young people, the heart rate increases and decreases when breathing in and out. These changes in heart rate are called respiratory sinus arrhythmia. This process is normal and requires no therapy. During sports, but also in everyday life, extra beats of the heart sometimes occur so-called extrasystoles. They are sometimes unpleasant, but usually harmless. In addition, a real athlete’s heart is sometimes so well trained that it can properly stimulate the circulation with fewer beats. This form of sinus bradycardia also has no disease value.
Diagnosis Of Heart Arrhythmia
The first contact person is usually a family doctor. He takes the first steps to get to the bottom of heart arrhythmia. For a more detailed clarification, however, he will refer you to a specialist for heart diseases, a cardiologist. In the beginning, the doctor asks the patient about his symptoms:
- Do you often feel dizzy? Have you ever collapsed?
- Are your hearts always racing? If so, how often and how long does an attack last?
- Does your heart often stumble?
- Do you experience breathing difficulties or chest pain from time to time?
The doctor is also interested in the patient’s medical history (in summary, the doctor takes a so-called anamnesis):
- What medications are you taking?
- Are you known to have a heart disease?
- Have you ever been treated for heart arrhythmias?
- Do you suffer from other diseases, for example, a thyroid gland dysfunction?
Then the doctor will examine you. He will take your blood pressure and feel your pulse. He will also listen to your heart.
Apparatus-based examinations
The doctor records the electrical activity of the heart and thus also heart arrhythmia with an electrocardiogram (ECG). Sometimes, however, patients suffer from temporary attacks of heart arrhythmia that do not occur during a visit to the doctor. In such cases, a long-term ECG examination is advisable, which records the heart’s actions continuously over a period of about 24 hours.
Under certain circumstances, heart arrhythmia does not occur during this period either. Then so-called event recorders can help. There are external and implantable recording devices. They automatically record heart arrhythmias that correspond to a certain pattern (this is programmed in beforehand). Some external devices also save the heart actions only at the push of a button, i.e. when the patient notices abnormalities.
Doctors use stress tests to determine how heart dysrhythmias behave during physical exertion. A bicycle ergometer is usually used for this purpose. In addition to the exercise ECG, this examination also includes measuring blood pressure. In addition, the examinations can be supplemented with a heart ultrasound (echocardiography).
Doctors often recognize underlying heart diseases in this. Under certain circumstances, these can also be seen in an X-ray of the chest. In some cases, the doctor will perform an electrophysiological examination. Within this framework, he can not only assess the heart arrhythmia well, but also treat it immediately if necessary (catheter ablation).
Heart Arrhythmias: What helps?
If a tachycardia situation occurs very suddenly, it is also possible to first try whether certain maneuvers slow down the pulse. For example, you can place an envelope of ice on your face or around your neck, or press with a held breath. This stimulates special sensors in the vessels. They give feedback to the central nervous system, which uses the vagus nerve to slow down heart activity.
Sometimes, however, doctors have to prescribe drugs that prevent or at least contain the heart rhythm disturbances. Depending on the type of heart dysrhythmia, they are taken permanently or only when the abnormal heartbeat occurs. Choosing the right medication is complex and depends on many factors. Known drugs that are used for heart arrhythmias
- Beta-blockers (generally control and lower the heart rate)
- Sodium channel blockers (especially flecainide as a “pill in the pocket” for seizure-like supraventricular tachycardia)
- Potassium channel blocker (e.g. amiodarone in atrial fibrillation)
- Calcium channel blocker (e.g. Verapamil)
- Digitalis (lowers atrial tachycardias, especially good if beta-blockers are not sufficient or low blood pressure does not allow the use)
- Parasympatholytics such as atropine or sympathomimetics such as orciprenaline (in bradycardias)
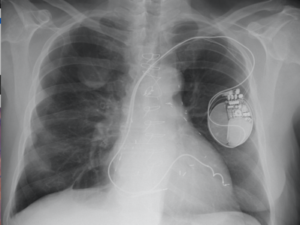
Sometimes patients need a pacemaker, a defibrillator or a device that contains both because of their heart arrhythmia. These devices are implanted under the skin. Wires run from there into the heart to deliver electrical impulses permanently or as needed. heart resynchronization therapy is used primarily in cases of severe heart insufficiency and left bundle branch block. With this device, two probes – one for each ventricle – cause the ventricles to beat again in the same rhythm.
Additional conduction pathways, for example in AV node reentry tachycardia, can be obliterated by doctors during an electrophysiological examination (high-frequency catheter ablation). This method often prevents renewed heart arrhythmias in the long term. However, treatment and prognosis depend not only on the type of disease but also on concomitant diseases and symptoms.
In addition, there are harmless heart arrhythmias (e.g. extrasystoles) that do not require treatment at all.